Ankle Sprains: Is it just a sprain?
The most common sports injury. But until you have had one, you do not realize how serious the injury can be. We see college and professional athletes get ankle sprains and sometimes come back to play the very next week. Hence, ankle sprains must not be that serious.
What we do not get to see with these high level athletes is the treatment that is initiated immediately after the injury by a team of trained sports medicine professionals. Daily treatments are performed, including physical therapy, bracing and taping, electrical stimulation, ice baths, etc., constituting the majority of the day for these high level athletes until they are ready to play.
For the high school level athlete and weekend warrior, these resources are limited. We rely on what our personal insurance will cover, as well as the high school trainers. Some schools have terrific training facilities, and others have none. This leaves the majority of the treatment in the hands of the athlete.
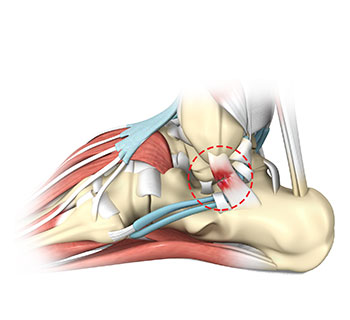
I would like to first clear-up some of the mystery behind ankle sprains. There is much confusion in the community about ankle sprains compared to torn ligaments. By definition, a sprain is an injury to a ligament or ligament complex. Ligaments stabilize joints, spanning across the joint from one bony attachment to another bony attachment. When a sprain occurs, the ligament is either stretched significantly or torn completely. Hence, "torn ligaments" are the very same as a sprain. There are grades of sprains, I through III, depending on the severity of the ligament damage. Ankle sprains similarly are graded, in some cases referred to as mild, moderate and severe. In many ankle sprains more than one ligament is damaged. The most common torn ligament in the human body is the anterior talofibular ligament of the lateral ankle.
Fortunately, the ankle is an inherently stable "hinge-type" joint. Thus, unlike the knee and shoulder, when ligaments are torn, surgery is rarely necessary. In fact, orthopedic research has confirmed that all grades of ankle sprains do well with non-operative care. This care initially involves the R.I.C.E. program, or rest, ice, compression and elevation. This requires patience, essentially resting the joint while icing and elevating until the swelling and bruising is under control. The most common mistake is not elevating it adequately, which should involve keeping the foot and ankle above heart and head 4 - 5 times a day for 20 minutes at a time. While the R.I.C.E. program is started, the second phase of treatment should be started, which includes early active rehabilitation weight-bearing as tolerated. This means graduating off crutches as soon as pain allows. Studies have shown that the quicker an athlete is able to bear weight on their sprained ankle, the better their outcome. Range of motion exercises should be started even while icing and elevating. Once the athlete is able to walk near normal and regains near normal range of motion, then the last phase of treatment can be started.
The last phase of treatment usually starts 2 - 3 weeks after the initial injury, and includes strengthening and proprioceptive retraining. The most common long-term problem with ankle sprains is the potential for recurrence. Up to 80% of athletes with sprains will re-sprain it at some point in their life. Proprioceptive retraining means teaching the body to recognize the position of the foot and ankle in space without using visual clues. This means balancing with the eyes closed.
All of the above treatments can be done at home, but the injury should be taken seriously. Initially, x-rays should be taken to rule out fracture, as often the presentation can be very similar. Formal physical therapy can assist in the above treatment program and provide many additional tricks to return the athlete to their sport quicker. I recommend early involvement of a sports medicine specialist, to review these x-rays and to initiate this therapy early.