Anterior Cruciate Ligament Reconstruction
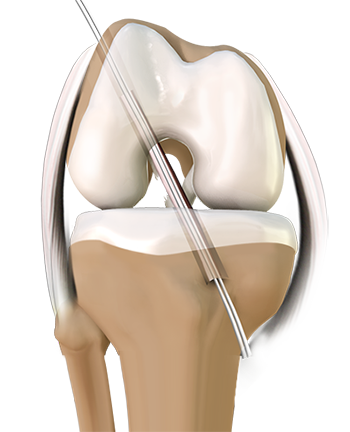
The main stabilizing ligament of the knee is the anterior cruciate ligament (ACL). It is centrally located in the knee joint, and is attached on the back side of the thigh bone (femur) and spans toward the front of the shin bone (tibia). Hence, it prevents the shin bone from shifting forward in relation to the thigh, especially when the knee is bent. It also prevents some external rotation of the shin bone, since it attaches from outside of the thigh bone toward the inside of the shin. When this ligament is torn or deficient, the knee will periodically feel as if it is actually dislocating or shifting abnormally.
This occurs frequently with quick stops and starts, or changes in direction. Pain and swelling can become common, due to the damage to other cartilage structures within the knee during the shifting. Many athletes will find that they are completely unable to perform with this injury, while others may have less frequent shifting episodes.
The current recommended treatment in young active people is surgical reconstruction. Without reconstruction, the knee is predisposed to shifting episodes, which leads to early arthritic problems. If activities are severely restricted, then reconstruction can be avoided. On the other hand, if the patient wants to continue a healthy, active lifestyle, then reconstruction is strongly encouraged. In fact, the younger the patient, the more strongly we encourage the need for surgery and reconstruction, as post-traumatic arthritis has been seen to develop very rapidly in even teenage patients.
The initial step after knee injury is to get to a Sports Medicine specialist for evaluation. In most cases, the integrity of the ligament can be determined by a combination of review of the mechanism of the injury and physical exam. X-rays and an MRI often complete the picture, and can help planning for surgery.
Surgical reconstruction is a major step. Even though it is an arthroscopic surgery, it is still a major surgery. There currently are many options for reconstruction, each with its own risks and benefits. The procedure and technique choices should be discussed thoroughly with the surgeon. Although the internet is a good source for information on the procedure, it is also a good source for misinformation. One common misunderstanding of the procedure is that the ligament can be primarily repaired. In fact, the ligament is usually destroyed in the injury and has to be replaced. What should be clarified with the surgeon is the choice of the graft replacement. Once that is determined, then an understanding of the graft fixation is needed. On average, considering the common graft choices and fixation techniques, the surgical success rate is greater than 90% at restoring stability to the knee.
A commonly overlooked element of the success of the surgery is the rehabilitation in the post-operative period. It has been considered that 80% of the success of the surgery is determined by the post-operative therapy, and strict compliance with the restrictions set by the surgeon. It should be expected that a period of 4 to 6 months without sports will be required after surgery, and elite level athletes have been found to need more in the neighborhood of 1 to 2 years to reach their pre-injury elite level.